A 15-Year Warranty Period for Asymptomatic Individuals Without Coronary Artery Calcium: A Prospective Follow-Up of 9,715 Individuals
Original Research
Abstract
Objectives
The aim of this study was to examine the long-term prognosis in asymptomatic individuals with a coronary artery calcium (CAC) score of 0 and its associated warranty period.
Background
Emerging evidence supports a CAC score of 0 as a favorable cardiovascular short-to intermediate-term prognostic factor.
Methods
A total of 9,715 individuals undergoing CAC imaging were stratified by age, Framingham risk score (FRS), and National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) categories and followed for a mean of 14.6 years (range 12.9 to 16.8 years). Cox regression, area under the receiver-operating characteristic curve, and net reclassification information were used to assess all-cause mortality, discrimination, and reclassification of a CAC score of 0 compared with the FRS and NCEP ATP III, respectively. A warranty period was pre-defined as <1% annual mortality rate. Vascular age was estimated by linear regression.
Results
In 4,864 individuals with a baseline CAC score of 0 (mean age, 52.1 ± 10.8 years; 57.9% male), 229 deaths occurred. The warranty period of a CAC score of 0 was almost 15 years for individuals at low and intermediate risk with no significant differences regarding age and sex. A CAC score of 0 was associated with a vascular age of 1, 10, 20, and 30 years less than the chronological age of individuals between 50 and 59, 60 and 69, 70 and 79, and 80 years of age and older, respectively. The CAC score was the strongest predictor of death (hazard ratio: 2.67, 95% confidence interval: 2.29 to 3.11) that enabled discrimination and consistent reclassification beyond the FRS (area under the receiver-operating characteristic curve: 0.71 vs. 0.64, p < 0.001) and NCEP ATP III (area under the receiver-operating characteristic curve: 0.72 vs. 0.64, p < 0.001).
Conclusions
A CAC score of 0 confers a 15-year warranty period against mortality in individuals at low to intermediate risk that is unaffected by age or sex. Furthermore, in individuals considered at high risk by clinical risk scores, a CAC score of 0 confers better survival than in individuals at low to intermediate risk but with any CAC score.
Introduction
In population-based studies, coronary artery calcium (CAC) scoring by computed tomography (CT) accurately stratifies cardiovascular risk in asymptomatic individuals (1–5). Notably, the presence (6,7), extent (8), and progression (9,10) of CAC have been shown to be associated with major adverse cardiovascular events (4,6–10) and death (3,4,10–15), independent of conventional risk factors. Conversely, a favorable prognosis has been observed in the absence of CAC (16–18). The majority of these studies have evaluated the beneficial effect of a CAC score of 0 in cohorts with up to 5 years of follow-up, a time point at which a generally low number of incident adverse clinical events has occurred. However, whether a CAC score of 0 confers long-term protection against poor survival incremental to and independent of clinical risk scoring and its associated “warranty period” remains to be elucidated. Further, several recent studies highlighted the important distinction between chronological age and “vascular age,” the latter of which adjusts an individual’s risk of mortality based on the level of CAC (19,20). To date, the long-term impact of a CAC score of 0 for the estimation of vascular age versus chronological age is unknown. Thus, in the present study, we set out to determine the long-term prognosis associated with a CAC score of 0, comparing the prognosis of a CAC score of 0 with the prognosis obtained by the current clinical prediction models such as the Framingham risk score (FRS) and the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III), quantifying the “warranty period” for a CAC score of 0, and, last, examining the association of a CAC score of 0 with chronological versus vascular age.
Methods
Study population
Study population
The study cohort comprised 9,715 consecutive asymptomatic individuals without known coronary artery disease (CAD). All individuals were referred by their physicians for CAD evaluation and underwent CAC imaging with electron beam computed tomography (EBCT) at a single site. All individuals provided informed consent to undergo EBCT, and the study was approved by the Human Investigations Committee at the Tennessee Heart and Vascular Institute.
Risk factor collection
All study participants were queried for the following baseline cardiovascular risk factors: 1) cigarette smoking was considered to be present if a subject was an active smoker at the time of scanning; 2) dyslipidemia was considered to be present for any individual reporting a history of high total cholesterol, high low-density lipoprotein cholesterol, low high-density lipoprotein cholesterol, high triglycerides, or current use of lipid-lowering therapy; 3) diabetes was defined as baseline use of antidiabetic medication or a history of elevated blood glucose measurement of >126 mg/dl; 4) hypertension was defined as a self-reported history of high blood pressure or the use of antihypertensive medication; and 5) family history of premature CAD was determined by asking individuals whether any member of their immediate family (i.e., parents or siblings) had a history of fatal or nonfatal myocardial infarction and/or coronary revascularization in a male relative younger than 55 years of age or a female relative younger than 65 years of age.
EBCT screening protocol
Subjects underwent EBCT on either a C-100 or C-150 Ultrafast CT scanner (Imatron, South San Francisco, California). With a tomographic slice thickness of 3 mm, a total of ∼40 sections were obtained beginning at the level of the carina and proceeding caudally to the level of the diaphragm. Images were obtained with a 100-ms/slice scanning time, with image acquisition electrocardiographically triggered at 60% to 80% of the R-R interval. A calcified lesion was defined as more than 3 contiguous pixels with a peak attenuation of at least 130 Hounsfield units. Each lesion was then scored using the method developed by Agatston et al. (21) (Agatston units). The estimated radiation dose was ∼1 mSv.
Study outcome
The primary endpoint of this study was death from all causes. Ascertainment of mortality status was conducted by individuals blinded to baseline historical data and EBCT results and was verified using the U.S. Social Security Death Index. The U.S. Social Security Death Index is a national registry of all deaths that have occurred in the United States, allowing for 100% mortality ascertainment among study participants.
Definition of warranty period
In accordance with society guidelines, an annual mortality rate <1% was used to define individuals as low risk (22). For the purposes of this study, a warranty period was defined as the time that an individual remained in the low-risk category; conversely, reported values of annual mortality rate higher than 1% signified warranty period cessation.
Statistical methods
Categorical variables are presented as count with proportion and continuous variables as mean ± SD. The Pearson chi-square test was used for comparison of categorical variables. Between-group comparisons of continuous variables were computed using the independent-samples Student t test or the Mann-Whitney U test, as appropriate. Multivariable Cox proportional hazard regression models reporting hazard ratios (HRs) with 95% confidence intervals (95% CIs) were performed to examine and compare the risk of death from all causes among individuals. The latter model adjusted for age, sex, cigarette smoking, and cardiovascular morbidities including diabetes, hypertension, dyslipidemia, and family history of premature CAD.
The relationship between a CAC score of 0 and mortality was determined as a function of varying cardiovascular risk as determined by widely used clinical risk scores. Cox regression models stratified individuals according to pre-defined categories as quantified by low (<10%), intermediate (10% to 20%), and high (>20%) risk using 10-year FRS and NCEP ATP III score (3,23).
Linear regression models were used to estimate the vascular age using patients’ chronological age as the dependent variable and the CAC score as the independent variable (19). Group differences between vascular age and chronological age were plotted. Additionally, for each corresponding category of age, annual mortality rates were calculated. The discriminatory power of the CAC score over FRS and NCEP ATP III was evaluated using the area under the receiver-operating characteristic curve (24) and compared using the DeLong method (25). Reclassification was determined using category-free net reclassification improvement indexes (26). Statistical analyses were performed using STATA version 12.0 (StataCorp LP, College Station, Texas) and SAS version 9.3 (SAS Institute Inc., Cary, North Carolina). A 2-tailed p value <0.05 was considered statistically significant.
Results
Study population
Study population
Of 9,715 individuals (mean age 53.4 ± 10.5 years, 59.3% male) undergoing CAC screening, 4,864 (mean age, 52.1 ± 10.8 years; 57.9% male) had a CAC score of 0. At a mean follow-up of 14.6 years (range 12.9 to 16.8 years), there were 936 (9.6%) deaths in the study population. Of the deaths, 229 (4.7%) and 707 (14.6%) occurred in individuals with CAC scores of 0 and >0, respectively. Demographic characteristics of the study sample are summarized in Table 1. Overall, hypertension, dyslipidemia, smoking status, diabetes, family history of premature CAD were more prevalent and FRS and NCEP ATP III were higher among individuals with a CAC score >0 versus a CAC score of 0. The survival rate was higher for those with a CAC score of 0 (95.1% vs. 83.7%, p < 0.001).
| Risk Factor Cohort | Overall (N = 9,715) | CAC = 0 (n = 4,864) | CAC >0 (n = 4,851) | p Value |
|---|---|---|---|---|
| Age, yrs | 53.4 ± 10.5 | 52.1 ± 10.8 | 54.6 ± 10.0 | <0.001 |
| Male | 59.3 | 57.9 | 60.8 | 0.003 |
| Hypertension | 43.4 | 36.8 | 50.1 | <0.001 |
| Dyslipidemia | 62.6 | 57.8 | 67.3 | <0.001 |
| Diabetes | 8.3 | 5.7 | 11.0 | <0.001 |
| Smoking | 39.3 | 33.6 | 45.0 | <0.001 |
| Family history of premature CAD | 68.7 | 69.7 | 67.7 | 0.03 |
| Death | 936 (9.6) | 229 (4.7) | 707 (14.6) | <0.001 |
| 15-year survival | 89.6 | 95.1 | 83.7 | <0.001 |
| FRS∗ | <0.001 | |||
| Low (<10%) | 40.7 | 50.0 | 31.4 | |
| Intermediate (10%–20%) | 41.3 | 37.3 | 45.3 | |
| High (>20%) | 18.0 | 12.7 | 23.3 | |
| NCEP ATP III† | <0.001 | |||
| Low (<10%) | 53.4 | 62.9 | 43.8 | |
| Intermediate (10%–20%) | 27.7 | 23.7 | 31.8 | |
| High (>20%) or DM | 18.9 | 13.4 | 24.4 |
CAC and long-term prognosis
On multivariable analyses, a CAC score >0 was the strongest predictor of death in the overall population beyond individual cardiovascular risk factors, FRS, and NCEP ATP III and was associated with a nearly 3-fold risk of death (HR: 2.67, 95% CI: 2.29 to 3.11) (Table 2). The presence of diabetes (HR: 2.53, 95% CI: 1.74 to 3.69), active smoking (HR: 1.95, 95% CI: 1.50 to 2.53), and hypertension (HR: 1.58, 95% CI: 1.21 to 2.06) were associated with an increased risk of mortality among individuals with a CAC score of 0. In the presence of any CAC, the risk increased proportionally with the severity in the CAC score but independently of the FRS and the risk model provided by the NCEP ATP III (Table 3). Men and women showed similar survival and mortality risk in either the presence or absence of CAC (Online Figures 1A and 1B).
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Overall (N = 9,715) | CAC = 0 (n = 4,864) | CAC >0 (n = 4,851) | ||||
| Univariable | Multivariable | Univariable | Multivariable | Univariable | Multivariable | |
| CAC >0 | 3.36 (2.89–3.90), p < 0.001 | 2.67 (2.29–3.11), p < 0.001 | NA | NA | NA | NA |
| Age | 1.04 (1.04–1.05), p < 0.001 | 1.04 (1.03–1.05) p < 0.001 | 1.03 (1.02–1.04), p < 0.001 | 1.03 (1.02–1.04), p < 0.001 | 1.05 (1.04–1.05), p < 0.001 | 1.05 (1.04–1.05), p < 0.001 |
| Female | 1.05 (0.93–1.20), p = 0.42 | 0.96 (0.84–1.09), p = 0.54 | 1.08 (0.83–1.40), p = 0.58 | 101 (0.78–1.32) p = 0.92 | 1.10 (0.94–1.27), p = 0.23 | 0.93 (0.80–1.09), p = 0.37 |
| Hypertension | 1.90 (1.67–2.16), p < 0.001 | 1.61 (1.41–1.84), p < 0.001 | 1.68 (1.30–2.18), p < 0.001 | 1.58 (1.21–2.06), p = 0.001 | 1.66 (1.43–1.94), p < 0.001 | 1.62 (1.39–1.89), p < 0.001 |
| Dyslipidemia | 0.81 (0.71–0.92), p = 0.002 | 0.69 (0.60–0.79), p < 0.001 | 0.93 (0.72–1.21), p = 0.60 | 0.83 (0.63–1.08), p = 0.16 | 0.66 (0.57–0.76), p < 0.001 | 0.65 (0.56–0.75), p < 0.001 |
| Diabetes | 2.98 (2.54–3.49), p < 0.001 | 2.22 (1.89–2.61), p < 0.001 | 2.84 (1.97–4.11), p < 0.001 | 2.53 (1.74–3.69), p < 0.001 | 2.48 (2.08–2.97), p < 0.001 | 2.15 (1.79–2.57), p < 0.001 |
| Family history of CAD | 0.75 (0.65–0.85), p < 0.001 | 0.76 (0.67–0.87), p < 0.001 | 0.93 (0.70–1.23), p = 0.61 | 0.93 (0.70–1.23), p = 0.61 | 0.71 (0.61–0.83), p < 0.001 | 0.71 (0.61–0.83), p < 0.001 |
| Smoking | 1.91 (1.68–2.17), p < 0.001 | 1.79 (1.58–2.04), p < 0.001 | 1.92 (1.48–2.48), p < 0.001 | 1.95 (1.50–2.53), p < 0.001 | 1.64 (1.41–1.90), p < 0.001 | 1.77 (1.52–2.05), p < 0.001 |
| Model 3 | Model 4 | |||||
| FRS, per 5% risk increase∗ | 1.21 (1.18–1.24), p < 0.001 | 1.17 (1.15–1.20), p < 0.001 | 1.17 (1.11–1.24), p < 0.001 | 1.18 (1.11–1.24), p < 0.001 | 1.17 (1.14–1.20), p < 0.001 | 1.17 (1.14–1.21), p < 0.001 |
| NCEP ATP III per 5% risk increase† | 1.29 (1.25–1.34), p < 0.001 | 1.23 (1.19–1.28), p < 0.001 | 1.28 (1.19–1.37), p < 0.001 | 1.28 (1.19–1.37), p < 0.001 | 1.21 (1.17–1.27), p < 0.001 | 1.22 (1.17–1.27), p < 0.001 |
| CAC Score | Overall (N = 9,715) | ||
|---|---|---|---|
| Univariable | Multivariable | ||
| Adjusted for FRS | Adjusted for NCEP ATP III | ||
| 0 | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) |
| 1–99 | 2.21 (1.86–2.64), p < 0.001 | 2.08 (1.74–2.48), p < 0.001 | 2.03 (1.70–2.42), p < 0.001 |
| 100–399 | 3.85 (3.19–4.66), p < 0.001 | 3.42 (2.83–4.14), p < 0.001 | 3.32 (2.74–4.02), p < 0.001 |
| 400–999 | 5.98 (4.84–7.39), p < 0.001 | 4.93 (3.98–6.12), p < 0.001 | 4.81 (3.87–5.97), p < 0.001 |
| ≥1,000 | 8.66 (6.79–11.05), p < 0.001 | 6.79 (5.29–8.72), p < 0.001 | 6.99 (5.46–8.95), p < 0.001 |
Warranty period of a CAC score of 0
Figure 1 describes the 15-year cumulative mortality rate in all study individuals and those considered at low risk by the FRS, NCEP ATP III, absence of CAD risk factors, and CAC score of 0; individuals with a CAC score of 0 had the lowest rates of mortality. Independent of FRS (Figure 2A) or NCEP ATP III (Figure 2B), a CAC score of 0 was associated with a favorable prognosis. Risk of all-cause mortality was higher in individuals with a CAC score >0 and low cardiovascular risk (FRS, HR: 3.3; 95% CI: 2.49 to 4.32; NCEP ATP III, HR: 3.09; 95% CI: 2.45 to 3.90) compared with those with a CAC score of 0 and high cardiovascular risk (FRS, HR: 2.8; 95% CI: 2.05 to 3.92; NCEP ATP III, HR: 2.94; 95% CI: 2.15 to 4.01).

The 15-Year Cumulative Mortality Rate for the Study Period
The 15-year cumulative mortality rate according to the overall study population (pink line) and individuals considered low risk by FRS (light blue line), NCEP ATP III (dark blue line), the absence of any coronary artery disease risk factor (yellow line), and CAC score of 0 (green line). CAC = coronary artery calcium; CV = cardiovascular; FRS = Framingham risk score; NCEP ATP III = National Cholesterol Education Program Adult Treatment Panel III.

Hazard Ratios for Risk of All-Cause Mortality
Hazard ratios for risk of all-cause mortality in individuals with and without CAC according to FRS (A) and NCEP ATP III (B). CIs = confidence intervals; other abbreviations as in Figure 1.
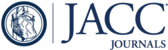
Figure 3 shows the annual mortality rates for individuals with CAC scores of 0 and >0. A CAC score of 0 was associated with a warranty period longer than 15 years, with the observed rate of mortality remaining <1% during the entire follow-up. Mortality rates in individuals with a CAC score of 0 were nonlinear in nature, with a lower event rate (0.3% ± 0.08% events/year) during the initial 12 years that accelerated during the 13th (0.4% events/year) and 14th (0.58% events/year) years. Figure 4 depicts the warranty period of a CAC score of 0 in select subgroups. A CAC score of 0 was associated with a warranty period of 15 years for individuals younger than 60 years of age, with no apparent disparity between sexes. The observed duration of the warranty period of a CAC score of 0 was slightly shorter for those 60 years of age and older and ceased after 14 years of follow-up. Despite a CAC score of 0, individuals considered at high cardiovascular risk by clinical risk experienced a significantly shorter warranty period (5 to 6 years) than individuals at low to intermediate risk. However, the warranty period for high-risk categories with a CAC score of 0 was even longer than for individuals at low to intermediate risk with a CAC score >0.

Annual Mortality Rate During the Study Period
An annual mortality rate <1% was used to classify individuals at low risk of cardiovascular events. CAC = coronary artery calcium.

Observed Warranty Period for the Absence of CAC Compared With the Presence of CAC
Observed warranty period (time to exceed 1% risk) for a CAC score of 0 compared with the presence of any CAC during 15 years of follow-up in 9,715 asymptomatic individuals stratified by CAC score, age, sex, FRS, and NCEP ATP III. Abbreviations as in Figure 1.
Vascular age in individuals with a CAC score of 0
A CAC score of 0 was associated with a lower vascular versus chronological age, a finding more pronounced for individuals of increasing age and for men versus women (Figure 5A). As an example, the vascular age afforded by a CAC score of 0 for a man 80 years of age and older was equivalent to the chronological age of a 50-year-old man in the general population. The annual mortality rate observed for patients with a CAC score of 0 was lower than the equivalent category of chronological age in the general population (Figure 5B).

Differences Between Chronological and Vascular Age
Differences between chronological versus vascular age in patients with a CAC score of 0 (A) and the corresponding annual mortality rate (B). CAC = coronary artery calcium.
Incremental predictive value of CAC for individuals with a CAC score >0
Compared with the base models of FRS or NCEP ATP III alone, discrimination improved significantly (area under the receiver-operating characteristic curve, 0.71 vs. 0.64 and 0.72 vs. 0.64 for FRS and NCEP ATP III, respectively; p < 0.001 for both) when the CAC score was added to the FRS or NCEP ATP III. The addition of the CAC score to the FRS or NCEP ATP III also resulted in significant reclassification of events and nonevents among individuals (both p < 0.001). Irrespective of risk prediction category, CAC score improved risk classification for those at risk versus not at risk of incident mortality (p < 0.001) (Table 4).
| NRI | 95% CI | p Value | % of Events Correctly Reclassified | Event p Value | % of Nonevents Correctly Reclassified | Nonevent p value | |
|---|---|---|---|---|---|---|---|
| Overall cohort (N = 9,715) | |||||||
| FRS + CAC | 0.58966 | 0.5251–0.6542 | <0.0001 | 29 | <0.0001 | 30 | <0.0001 |
| NCEP ATP III + CAC | 0.57966 | 0.5149–0.6444 | <0.0001 | 28 | <0.0001 | 30 | <0.0001 |
| Low cardiovascular risk | |||||||
| FRS + CAC | 0.52561 | 0.3961–0.6551 | <0.0001 | 12 | 0.07 | 41 | <0.0001 |
| NCEP ATP III + CAC | 0.49967 | 0.3878–0.6116 | <0.0001 | 13 | 0.02 | 37 | <0.0001 |
| Intermediate cardiovascular risk | |||||||
| FRS + CAC | 0.46417 | 0.3611–0.5672 | <0.0001 | 23 | <0.0001 | 23 | <0.0001 |
| NCEP ATP III + CAC | 0.51544 | 0.3955–0.6354 | <0.0001 | 28 | <0.0001 | 23 | <0.0001 |
| High cardiovascular risk | |||||||
| FRS + CAC | 0.58347 | 0.4709–0.6961 | <0.0001 | 40 | <0.0001 | 18 | <0.0001 |
| NCEP ATP III + CAC | 0.55956 | 0.4494–0.6698 | <0.0001 | 37 | <0.0001 | 19 | <0.0001 |
Discussion
In the present study, we extensively examined the long-term prognostic utility of CAC imaging in a large cohort of asymptomatic individuals with 15 years of follow-up. We observed the presence of CAC to be a strong predictor of incident mortality, even when considering robust clinical risk scores by FRS or NCEP ATP III methods. Importantly, we identified a very low risk state that lasted for the duration of follow-up. The low risk associated with a CAC score of 0 persisted for more than 15 years for individuals younger than 60 years of age and for 14 years for individuals 60 years of age and older, with no apparent disparity among sexes. Importantly, the warranty period conferred by a CAC score of 0 was similar for individuals at low- or intermediate-clinical risk by the FRS and NCEP ATP III. Individuals considered at high clinical risk but with a CAC score of 0 had a longer warranty period than those at low- or intermediate-clinical risk with any CAC score. Conversely, the presence and severity of CAC were independently associated with increased mortality risk by the FRS and the NCEP ATP III. Finally, a CAC score of 0 was associated with a vascular age that was ∼30 years lower than chronological age for older individuals and was associated with a significantly lower annual mortality rate than the equivalent chronological age category. Taken together, these findings indicate the robustness of a CAC score of 0 to identify individuals disposed to a particularly propitious outcome and may be useful as an adjunctive measure for everyday clinical risk assessment.
The present findings support and expand the extant literature (16–18) on studies that investigated the incremental utility of CAC imaging for the evaluation of asymptomatic individuals at risk of cardiovascular disease. The high prevalence of a CAC score of 0 in individuals classified as intermediate to high risk based by clinical risk scores suggests that such scores are highly imperfect in identifying persons at increased risk of mortality (27,28). To this end, the present study detected a significantly higher risk of mortality for individuals with a CAC score >0 who were considered at low risk by clinical score with respect to those with a CAC score of 0 who were considered at intermediate or high risk. Yet, although robust in risk prediction, a CAC score of 0 was significantly less effective at conferring a long-term warranty for individuals considered high risk by the FRS and NCEP ATP III. Thus, although current guidelines support the use of CAC imaging in asymptomatic individuals at intermediate cardiovascular risk (29), the present study suggests a long-term incremental value of a CAC score >0 for individuals initially considered to be at low risk but who are subsequently reclassified as at high cardiovascular risk based on CAC testing. Whether there is a clinical benefit of identification of a shorter warranty period of 5 to 6 years for individuals considered to be at high risk by FRS or NCEP ATP III requires further examination in health outcomes studies.
In this study, the beneficial prognosis of a CAC score of 0 is further supported by evidence of a vascular age reduction compared with chronological age, with an associated improvement in prognosis. Although it is generally accepted that the prevalence of coronary plaque burden and mortality rate increase with advancing age, the presence of a CAC score of 0 may be effective as an index of “vascular youth” (19,20). These study findings validate the concept of “vascular youth,” as determined by a CAC score of 0, in which individuals older than 50 years of age may be reassured that their coronary vasculature is “younger” than that of their peers and that this auspicious finding confers a good long-term prognosis.
These study findings are of high clinical importance. Given the 15-year warranty of a CAC score of 0 for individuals at low to intermediate clinical risk irrespective of sex and age—a period only slightly attenuated for patients 60 years of age and older—the use of CAC may be instrumental for avoiding unnecessary testing, even in individuals generally considered at higher risk of unexpected adverse clinical events. Although some may speculate that the prognostic security of a CAC score of 0 may offer an opportunity to attenuate medical therapies, our study findings apply only to coronary rather than cardiovascular assessment in other vascular beds such as the carotid circulation. Thus, the present results should not be interpreted as supporting a practice of therapy diminution or cessation as this matter is beyond the scope of our investigation. Future large-scale studies examining this concept should first be performed.
Study limitations
This study is not without limitations. Despite the large study sample size, long-term follow-up, and prospective evaluation of study individuals, the single-center design of the present study may have introduced unobserved biases related to selection. In this regard, future population-based studies with long-term follow-up will be important to help confirm the present study findings. Further, CAC imaging was performed only once for the present study, and the rates of CAC progression were not accounted for in the determination of the warranty period of a CAC score of 0. It remains conceivable that individuals who experience accelerated or retarded CAC progression may have different warranty periods, and future studies should be performed to examine this. Also, the long-term mitigating effects of medical therapy and lifestyle modification and how they might influence the relationship between CAC and mortality cannot be accounted for in this investigation. Hence, future studies that use time-varying clinical measures in patients with known CAC values are now needed. Finally, we used all-cause mortality as the primary endpoint for this study, and, thus, our analysis is unable to offer information regarding the impact of CAC specifically on cardiovascular morbidity and mortality, such as that used for the 2013 American College of Cardiology/American Heart Association guidelines (30). However, the use of mortality disentangles the study from ascertainment or misclassification bias and represents the most difficult endpoint to be evaluated in population studies. Indeed, the lack atherosclerotic cardiovascular disease–specific mortality in our study may have only contributed to an underestimation of the real impact of CAC on cardiovascular risk (31).
Conclusions
A CAC score of 0 confers a 15-year warranty period against mortality that is unaffected by age or sex, with a significant reduction in vascular rather than chronological age. These findings are consistent in individuals at low and intermediate risk. In individuals considered at high risk by clinical risk scores, the presence of a CAC score of 0 confers a longer warranty period compared with individuals at low or intermediate risk in the presence of any CAC.
Perspectives
COMPETENCY IN MEDICAL KNOWLEDGE: Traditionally, CAD has been assessed in terms of measures of stenosis severity. Characterization of atherosclerotic plaque characteristics, in addition to stenosis severity, may improve the diagnosis and prognostic risk assessment of patients with CAD. Features suggesting high-risk as seen with computed tomography include atherosclerotic plaque and coronary artery calcification volume and density and others, such as low attenuation plaque, positive remodeling, and spotty calcification. Conversely, the absence of CAC is protective against coronary events during long-term follow-up.
TRANSLATIONAL OUTLOOK: Additional clinical studies are required to determine the optimal methods for reporting CAD measures of stenosis or atherosclerosis, as well as to determine their prognostic implications and optimal approaches to therapy.
Abbreviations and Acronyms
| CAC | coronary artery calcium |
| CAD | coronary artery disease |
| CI | confidence interval |
| CT | computed tomography |
| EBCT | electron beam computed tomography |
| FRS | Framingham risk score |
| HR | hazard ratio |
| NCEP ATP III | National Cholesterol Education Program Adult Treatment Panel III |
References
1. "Cardiovascular imaging for assessing cardiovascular risk in asymptomatic men versus women: the multi-ethnic study of atherosclerosis (MESA)". Circ Cardiovasc Imaging 2011;4:8-15.
2. "Coronary artery calcium score and coronary heart disease events in a large cohort of asymptomatic men and women". Am J Epidemiol 2005;162:421-429.
3. "Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality". Radiology 2003;228:826-833.
4. "Coronary artery calcification compared with carotid intima-media thickness in the prediction of cardiovascular disease incidence: the Multi-Ethnic Study of Atherosclerosis (MESA)". Arch Intern Med 2008;168:1333-1339.
5. "ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography". J Am Coll Cardiol 2007;49:378-402.
6. "Coronary calcium as a predictor of coronary events in four racial or ethnic groups". N Engl J Med 2008;358:1336-1345.
7. "Severity of coronary artery calcification by electron beam computed tomography predicts silent myocardial ischemia". Circulation 2000;101:244-251.
8. "Progression of coronary artery calcium predicts all-cause mortality". J Am Coll Cardiol Img 2010;3:1229-1236.
9. "Annual progression of coronary artery calcium by spiral computed tomography in hypertensive patients without myocardial ischemia but with prominent atherosclerotic risk factors, in patients with previous angina pectoris or healed acute myocardial infarction, and in patients with coronary events during follow-up". Am J Cardiol 2001;87:1395-1397.
10. "Electron-beam tomography coronary artery calcium and cardiac events: a 37-month follow-up of 5635 initially asymptomatic low- to intermediate-risk adults". Circulation 2003;107:2571-2576.
11. "Risk stratification in uncomplicated type 2 diabetes: prospective evaluation of the combined use of coronary artery calcium imaging and selective myocardial perfusion scintigraphy". Eur Heart J 2006;27:713-721.
12. "Prognostic value of coronary artery calcium screening in subjects with and without diabetes". J Am Coll Cardiol 2004;43:1663-1669.
13. "Coronary calcium predicts events better with absolute calcium scores than age-sex-race/ethnicity percentiles: MESA (Multi-Ethnic Study of Atherosclerosis)". J Am Coll Cardiol 2009;53:345-352.
14. "Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals". JAMA 2004;291:210-215.
15. "Mortality rates in smokers and nonsmokers in the presence or absence of coronary artery calcification". J Am Coll Cardiol Img 2012;5:1037-1045.
16. "Diagnostic and prognostic value of absence of coronary artery calcification". J Am Coll Cardiol Img 2009;2:675-688.
17. "Prognostic significance of zero coronary calcium scores on cardiac computed tomography". J Cardiovasc Comput Tomogr 2007;1:155-159.
18. "Absence of coronary artery calcification and all-cause mortality". J Am Coll Cardiol Img 2009;2:692-700.
19. "Coronary artery calcium as a measure of biologic age". Atherosclerosis 2006;188:112-119.
20. "Calculation of coronary age using calcium scores in multiple ethnicities". Int J Cardiovasc Imaging 2008;24:107-111.
21. "Quantification of coronary artery calcium using ultrafast computed tomography". J Am Coll Cardiol 1990;15:827-832.
22. "ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients With Chronic Stable Angina)". J Am Coll Cardiol 1999;33:2092-2197.
23. "Prediction of coronary heart disease using risk factor categories". Circulation 1998;97:1837-1847.
24. "Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond". Stat Med J 2008;27:157-172.discussion 207–12.
25. "Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach". Biometrics 1988;44:837-845.
26. "Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers". Stat Med 2011;30:11-21.
27. "Coronary risk stratification, discrimination, and reclassification improvement based on quantification of subclinical coronary atherosclerosis: the Heinz Nixdorf Recall study". J Am Coll Cardiol 2010;56:1397-1406.
28. "Coronary artery calcium score and risk classification for coronary heart disease prediction". JAMA 2010;303:1610-1616.
29. "AHA Guidelines for Primary Prevention of Cardiovascular Disease and Stroke: 2002 Update: Consensus Panel Guide to Comprehensive Risk Reduction for Adult Patients Without Coronary or Other Atherosclerotic Vascular Diseases. American Heart Association Science Advisory and Coordinating Committee". Circulation 2002;106:388-391.
30. "2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines". J Am Coll Cardiol 2014;63:2889-2934.
31. "Cause of death in clinical research: time for a reassessment?"J Am Coll Cardiol 1999;34:618-620.
Appendix
Online Figure 1Footnotes
This study was supported in part by grants from the National Institutes of Health (R01HL115150 and R01HL118019) and also funded in part by a generous gift from the Dalio Institute of Cardiovascular Imaging and the Michael Wolk Foundation. Dr. Truong is supported by NIH grants K23HL098370 and L30HL093896 and has received grant support from St. Jude Medical, American College of Radiology Imaging Network, and Duke Clinical Research Institute. Dr. Chang is supported by Leading Foreign Research Institute Recruitment Program through the National Research Foundation of Korea funded by the Ministry of Science, ICT, & Future Planning (MSIP) grant 2012027176. Dr. Min has served on the medical advisory boards of GE Healthcare, Arineta, AstraZeneca, and Bristol-Myers Squibb; on the Speakers Bureau of GE Healthcare; received research support from GE Healthcare, Vital Images, and Phillips Healthcare; serves as a consultant to AstraZeneca, Abbott Vascular, HeartFlow, NeoGraft Technologies, MyoKardia, and CardioDx; and is supported by grants NIH/NHLBI-R01 HL111141, NIH/NHLBI-R01 HL115150, NIH/NHLBI-R01 HL118019, NIH/NHLBI-U01 HL105907, and a grant from the Qatar National Research Foundation NPRP09-370-3-089. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Sherif Nagueh, MD, served as Guest Editor for this paper.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}